Tarsal ectropion: when the lower eyelid turns inside out
One of the more dramatic eyelid problems I see, and one of the most often missed. Why it happens, why it is so common in men, and how a combined repair addresses all three parts of the problem.
A gentleman in his eighties came to my clinic having put up with red, sore, sticky eyes for years. The pink lining of both his lower eyelids was hanging visibly outwards. He had tried lubricant drops, antibiotic ointments, and reassurance, none of which had touched the problem. Two weeks of steroid ointment, a single operation, and a fortnight of healing later, his eyes were comfortable for the first time in a decade.
This is tarsal ectropion. It is one of the more dramatic eyelid problems I see, and one of the most often missed.
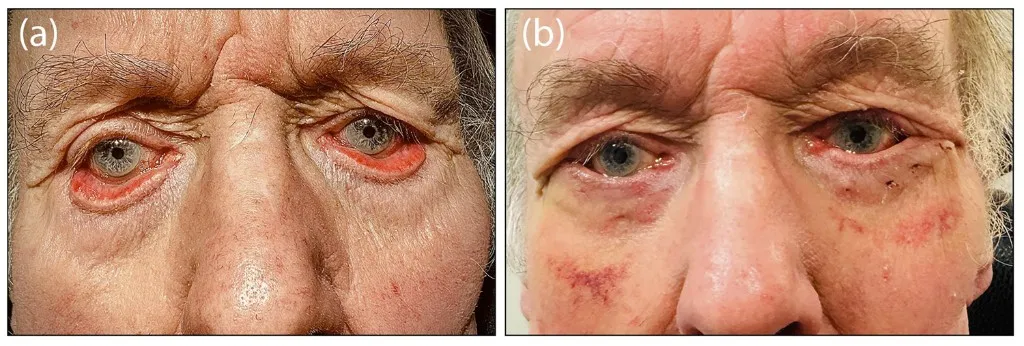
Figure 1. Photographs of a patient undergoing lateral tarsal strip, sub-orbicularis oculi fat lift and lower eyelid retractor plication with Tse inverting sutures for bilateral tarsal ectropion. Images are taken immediately preoperatively following a 2 week course of topical steroid ointment (a), and 2 weeks postoperatively (b). In the preoperative image (a), one can observe the mid face descent and clear disassociation of the anterior and posterior lamellae of the eyelid.
Reproduced with permission from Rosen H, Ben Ishai M, Radhalakshmi A, Oliphant H, Rajak S, Schulz C. An evaluation of surgical outcomes following tarsal ectropion repair: a multi-centre retrospective cohort study. European Journal of Ophthalmology. 2026;36(2):371–378. doi:10.1177/11206721251383991
What is going on
Think of the lower eyelid as a folded piece of paper. The fold sits at the lid margin, where the skin on the outside meets the pink lining (the conjunctiva) on the inside. Tucked inside the fold is the tarsus, a small firm plate that gives the lid its shape. Two things hold the structure together: a strong attachment at the lid margin, and a sheet of muscle and fascia behind the lid, called the retractors, which behave like glue between the two folded sides.
In tarsal ectropion, the retractors give way. The two sides of the fold lose their adhesion. The eyelid unfolds and the pink lining is left facing outwards, exposed to the air.
Once exposed, the lining quickly becomes inflamed. It thickens, swells, and produces a sticky mucous discharge. The swelling itself makes it harder for the lid to return to its normal position, and the cycle continues. By the time most patients reach me, they have been living with this for years.
Why it tends to happen in men
Around 70 percent of the patients in our recent study were men, which matches what other groups have found in much larger populations. The reasons are anatomical.
Women tend to have a thicker, more padded mid cheek, which acts as a natural cushion supporting the lower eyelid from below. Men have less of this padding to start with. As the cheek descends with age, in men there is very little to resist the downward pull on the eyelid skin. Years of sun exposure, typically greater in men, weaken the skin further and erode its connections to the structures behind it.
Men also tend to have larger tarsal plates, which means more leverage on a structure that is already losing its support. The combination of a heavier lid, less cushioning, more sun damage, and the same age-related retractor weakness adds up to a higher risk.
Why it sometimes gets misdiagnosed
Because the eyelid skin looks stretched, it is sometimes assumed that there is a shortage of skin, and a skin graft is offered. In most cases this is the wrong answer. The skin is not actually short. It has been pulled out of position by the descending cheek. A skin graft alone does not solve the underlying problem and often leaves a worse cosmetic result.
What helps far more is lifting the cheek back up and re-establishing its connection to the supporting tissues. The skin then sits where it is supposed to, and the eyelid can fold back into shape.
How I treat it
There is no single operation that suits everyone, and a careful examination is essential before deciding on the plan. My approach addresses all three elements of the problem in the same operation:
- Tighten the eyelid at the outer corner. I usually do this with a lateral tarsal strip, which restores the firm anchor of the lid against the bone of the orbit.
- Reattach the retractors and lift the cheek. I use a SOOF lift (sub-orbicularis oculi fat lift) together with a stitch technique called Tse inverting sutures, which I adapted from the published work of Dr David Tse. These sutures pull the eyelid back into its folded shape and re-anchor the front of the lid to the retractors behind. This is the part that most often gets missed.
- Settle the inflammation. I usually prescribe a course of steroid ointment for two to four weeks before surgery. This reduces the conjunctival swelling so the lid can return to its normal position more easily. The ointment is continued for a further two weeks after the operation.
In our recent multi-centre study (Rosen et al., European Journal of Ophthalmology, 2025, PubMed link), we showed that combining horizontal and vertical correction reduced recurrence by more than three-fold compared with horizontal tightening alone. Patients who had perioperative steroid drops or ointment had around a 60 percent lower risk of recurrence.
What to expect after surgery
The eye is usually sore and swollen for the first week, and there is some bruising. By two weeks most patients are comfortable, the redness has begun to settle, and the sticky discharge is gone. By six weeks the result is usually settled.
Recurrence remains possible. Our study found that around a third of patients had some degree of partial recurrence in the longer term, though most of these were minor and caused little symptomatic trouble. Being honest about this is important, and is one of the reasons we are studying this carefully and continuing to refine the technique.
When to seek a second opinion
If your eyelid has been chronically red and sticky despite drops, if you have been told the only option is a skin graft, or if previous ectropion surgery has not held, it is worth being assessed by an oculoplastic surgeon who treats this condition routinely. Tarsal ectropion is uncommon enough that not every general ophthalmologist sees many of them, and the pattern of the problem is easily missed.